Home /
Expert Answers /
Nursing /
required-information-the-following-information-appires-to-the-questions-displayed-below-the-objec-pa435
(Solved): Required information [The following information appires to the questions displayed below] The objec ...
Required information [The following information appires to the questions displayed below] The objective of these exercises is to correctly complete TRICARE claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. Billing Provider Information Name: Valley Associates, PC Address: 1400 West Center Street Toledo, Telephone: 555.967.0303 Employer ID Number: NPI: 1476543215 Rendering Provider Information Name: Nancy Ronkowski, MD NPI: 9475830260 Assignment: Accepts Signature: On File (01/01/2029)
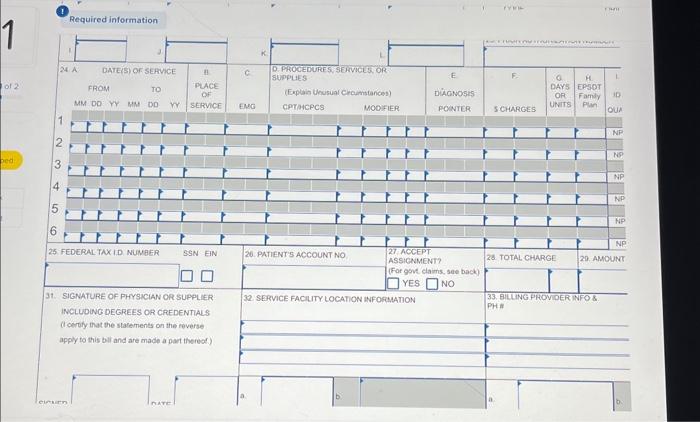
Want to enter information. For the purposes of Connect, all dates should be entered in 8 -digit format (XX in MM field: in DD field, XXXXX in YY field) except for Item Number 24, where the dates should be entered in 6 -digit format (XX in MM field, in field; in YY field). NOTES: this medical facility does not use an outside lab; the patient's chart number should be used for the patient account number; we have tried to include information you might need from earlier Case Studies, but please refer back to Chapter 7 if necessary. Click on the link below to access the Encounter Form. Encounter Form Information About the Patient: Name: Sylvia Evans Sex: F Birth Date: 06/10/1987 Marital Status: Married Address: 13 Ascot Way Sandusky, 44870-1234 Telephone: Employer: United States Army Race: White Ethnicity: Not Hispanic or Latino Preferred Language: English nsured: Self Health Plan: TRICARE Number: 140396602 olicy Number: N/A to TRICARE
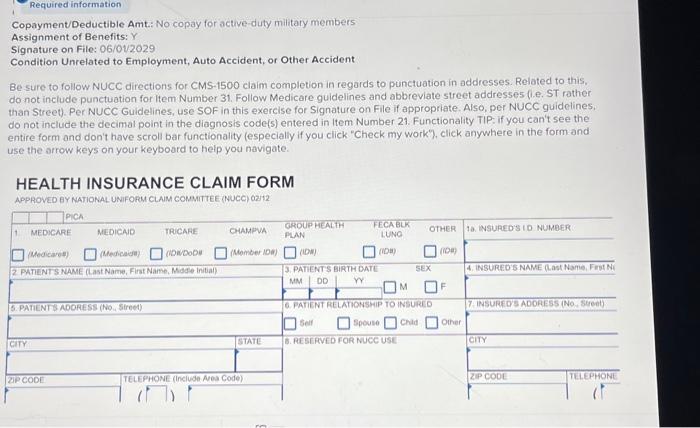
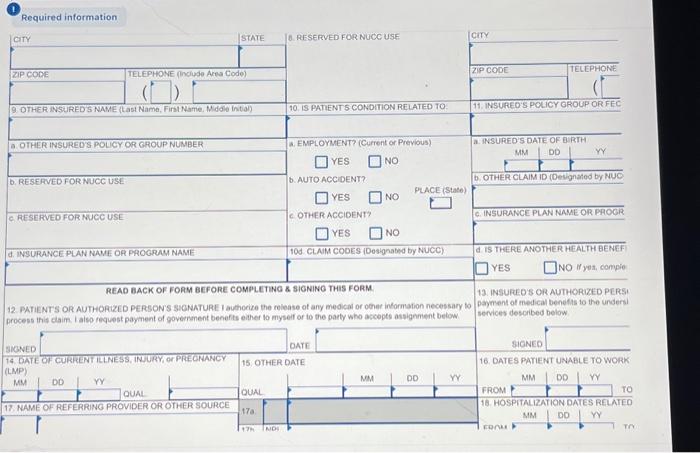
Copayment/Deductible Amt: No copay for active-duty military members Assignment of Benefits: Y Signature on File: 06/01/2029 Condition Unrelated to Employment, Auto Accident, or Other Accident Be sure to follow NUCC directions for CMS-1500 claim completion in regards to punctuation in addresses. Related to this. do not include punctuation for item Number 31. Follow Medicare guidelines and abbreviate street addresse5 (1.e. ST rather than Street). Per NUCC Guidelines, use SOF in this exercise for Signature on File if appropriate. Also, per NUCC guidelines. do not include the decimal point in the diagnosis code(s) entered in Item Number 21. Functionality TIP: if you can't see the entire form and don't have scroll bar functionality (especially if you click "Check my work"), click anywhere in the form and use the arrow keys on your keyboard to help you navigate. HEALTH INSURANCE CLAIM FORM APPROVEO EY NATIONAL UNIFOPM CLAM COMMITTEE (NUCC) 02212
(1) Required information
(1) Required information